-01")
Member Only Post
By Francisco Eraso, DDS, MS, MS, MSD
Orthodontic practitioners are continually looking for ways to be more efficient. When the worldwide pandemic hit, the workflow in my practice included advanced appliances, 3D CBCT imaging, digital photographs and intraoral scanning so it was digitally based and quite efficient. Even with all that, I still found myself asking how I could maximize the technologies I currently employed and/or what others I should add to meet my patient’s heightened expectations.
With COVID-19 cases quite prevalent, my patients who had already been finding it challenging to fit appointments into their hectic schedules, were now reluctant to make in-office visits for fear of infection. Add inflation into the mix, particularly with gas prices what they are, and we had to ask ourselves, “How could we adapt?” What systems would allow us to “see” patients who felt uncomfortable coming into the office and still care for them properly while providing a positive and comfortable patient experience?
A philosophy called Minimum Touch OrthodonticsSM (MTO) is one that makes sense to me. Henry Schein Orthodontics™ launched the concept under the guidance of its orthodontist advisors. The idea of MTO is to assist clinicians in focusing their efforts on delivering simplified, predictable results in fewer and shorter appointments in minimal overall treatment time. The ultimate goal is to maximize convenience and enhance the overall patient experience, capitalizing on advanced appliances and digital technologies.
Same-Day Starts Satisfy Patient Needs
A good place to begin discussing MTO is with Same-Day Starts. You likely have longstanding relationships with most of your prospective orthodontic patients so a Same-Day Start may not be as off-putting to you as it first was to many specialists. When I initially heard about the idea, I was concerned patients would feel rushed. When a patient mentions to you the prospect of undergoing orthodontics, accommodating them in the schedule for taking records that day—or at least getting a contract signed or a follow-up appointment scheduled—precludes their needing to return for another appointment, going for a second opinion or opting for a “DIY” (do it yourself) remedy. With the pandemic still lingering in places and gas prices what they are, Same-Day Starts make sense and are the foundation for a satisfying patient experience.
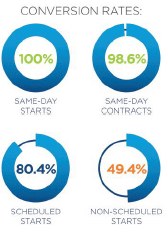
OrthoFi1 reports that for specialists’ offices, conversion rates of Same-Day Starts—defined as records being taken or any appliance being bonded—drops only 1.4% if a contract is secured same day. Even if the start appointment is scheduled, conversion rates drop only 20% but plummet over 50% if no next appointment is scheduled (Fig. 1). The key to garnering solid patient commitment, then, is securing a contract, taking records or bonding an appliance without compromising the most optimal diagnosis and treatment planning.
Making Same-Day Starts Practical
The solution that makes Same-Day Starts practical is the Carriere® Motion 3D™ Appliance for sagittal correction (both CL II and CL III). Since sagittal correction is required for a large proportion of orthodon-tic cases, being able to get the A/P correction started at the exam appointment just after records are taken appeals to patients’ need for convenience, ensuring clinical efficiency and case conversion.

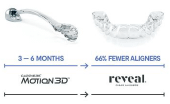
The Motion Appliance (Fig. 2) is used to establish a Class I platform prior to completing treatment with either aligners or braces. It simplifies finishes and can reduce overall treatment time, including the number of aligners employed (Fig. 2a). In terms of adopting Minimum Touch Orthodontics and keeping conversion rates high, I strongly believe the Motion Appliance is an essential tool.
While just over half of orthodontists continue to use a rigid, fixed functional appliance for skeletal Class II correction, and nearly 75% of those use a Herbst-type appliance2, I have found Motion to be effective for both CL II and CL III correction. In my practice, it takes approximately five minutes of chair time to bond and there is minimal doctor time for a proper diagnosis and treatment plan to indicate its use. We use our in-house 3D printer to deliver the opposite arch aligner for anchorage the same day. The mess and delay of delivering a Herbst-type appliance are no longer issues.
Presenting the Motion Appliance versus a Herbst to prospective patients is obviously much easier. With the Motion Appliance, patients who are undecided about whether to complete treatment in braces or aligners need not make the decision until after the sagittal correction. The Sagittal First philosophy, on which the Motion Appliance is based, means there are no competing forces in the mouth during A/P correction. Motivated patients are usually compliant. Adults who have just invested in treatment are highly motivated and even adolescents are usually so eager to get their braces or aligners so they, too, wear their Motion elastics as they should.
Effective and Efficient Class II Correction
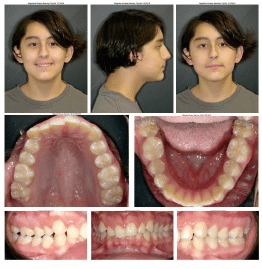
Case 1 (Fig. 3) demonstrates the use of the Motion Appliance in a young man in permanent dentition at age 13 years, 9 months. He presented as CL II (dental and skeletal), with a deep bite, mild occlusal cant and mild to moderate crowding in each arch.
The patient was bonded with the Carriere Motion CL II Appliance at the exam appointment. The anterior of the pads were bonded to the canine on the left and to the first premolar on the right so the right canine would fully extrude as the posterior segment distalized. The posterior pads were bonded to the upper first molars (usual protocol). Carriere® Oral Elastics-Force 1 (HSO, Carlsbad, CA) were engaged from the anterior pads to the Carriere® Motion™ 3D Sidekick™ bondable hook secured to the buccal of the lower second molars for the first week. Force 2 elastics (HSO, Carls-bad, CA) were engaged for the remainder of sagittal treatment.

Bondable buttons, buccal tubes or molar bands are also options for lower second molar engagement. An Essix-type retainer fabricated in house provided anchorage in the opposite arch (not pictured.) After five months (Fig. 4), the molars had corrected to CL I with the canines overcorrected by ¼ cusp (super CL I platform) to ensure they would end in the proper position.
The full content of this page is only visible to AOS Memberships with digital Journal Access. You can view the full content of this page by signing up for a qualifying AOS Membership. Our Doctor Membership is just $41.67 per month, billed annually. Use the links below to learn about all of our membership benefits and features.
